About the DAMNIT-V Screen
Clinical Utility Demonstrated Over Time
Quick Definition
What it is:
Non-contact functional screening and clinical decision-support tool.
What it measures:
Patient autonomic response patterns during exposure to DAMNIT-V–aligned test domains (RAC-type events).
What it’s for:
Prioritising investigative direction in complex or unclear cases.
What it is not:
A diagnostic test.
Diagnosis always requires standard veterinary diagnostics.
Purpose and Clinical Role
The DAMNIT-V Screen was developed through long-term use in everyday veterinary practice as a functional screening tool to assist clinical prioritisation.
It does not replace:
- Pathology
- Imaging
- Laboratory testing
- Histopathology
- Culture
Its defined purpose is:
To improve clinical clarity at the time of assessment.
The system assesses physiological response behaviour to defined test domains aligned with the DAMNIT-V framework. These responses are interpreted in context, alongside history, examination, and conventional diagnostics.
Why It Was Developed
Many veterinary cases do not present with a single, clearly localised pathology. Instead, clinicians frequently encounter:
- Overlapping signs
- Multi-system involvement
- Early or subclinical dysfunction
- Non-specific presentations
Before committing to sequential or invasive diagnostics, the practical question is often:
Where should I investigate first?
The DAMNIT-V Screen was designed to help address that question by providing structured functional context.
What the System Measures
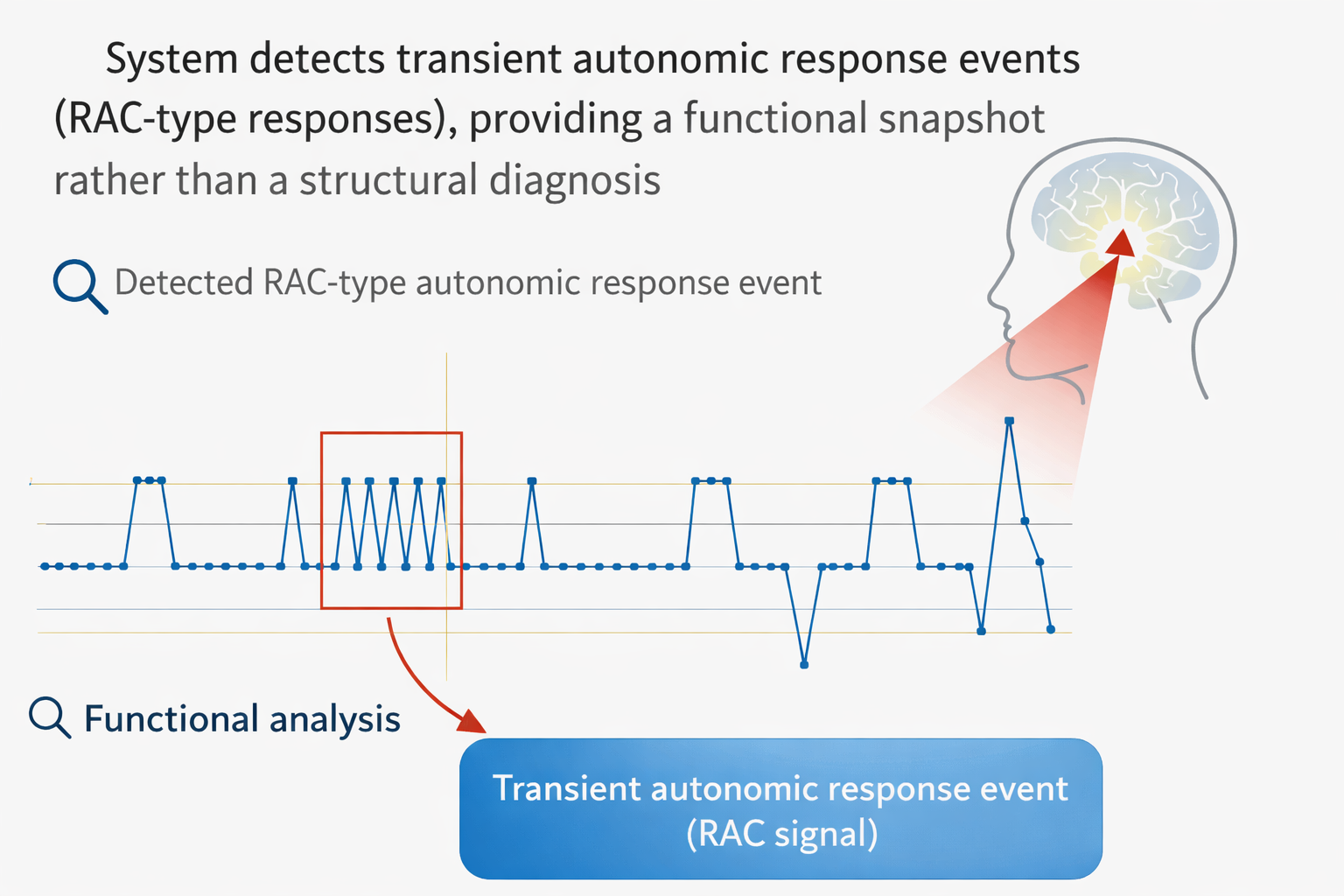
The DAMNIT-V Screen records transient autonomic response events (RAC-type responses) during exposure to defined test domains.
It does not detect:
- Pathogens
- Hormones
- Toxins
- Structural lesions
- Genetic abnormalities
It evaluates host physiological reactivity at the time of testing.
Output and Interpretation
RAC Event Count
Results are expressed as the number of Reflex Auriculo-Cardiac (RAC) responses detected during a standardised 5-second exposure period.
A RAC event is a reproducible transient autonomic response pattern detected by the system.
Interpretive Guidance (Practice-Derived)
Under standard operating conditions:
- 0–10 events: Background physiological variation
- 11–20 events: Mild response; interpret clinically and confirm repeatability
- 21–30 events: Response warranting further targeted investigation
- >30 events: Strong response; conventional diagnostics indicated
These are interpretive guides based on clinical experience.
They are not validated diagnostic thresholds.
Evidence and Validation
Practice-Based Longitudinal Dataset (2014–2025)
The most complete dataset relates to cranial cruciate ligament (CCr) disease in desexed dogs.
This model was selected because:
- CCr disease is common
- It is multifactorial
- Endocrine influences have been proposed in pathogenesis
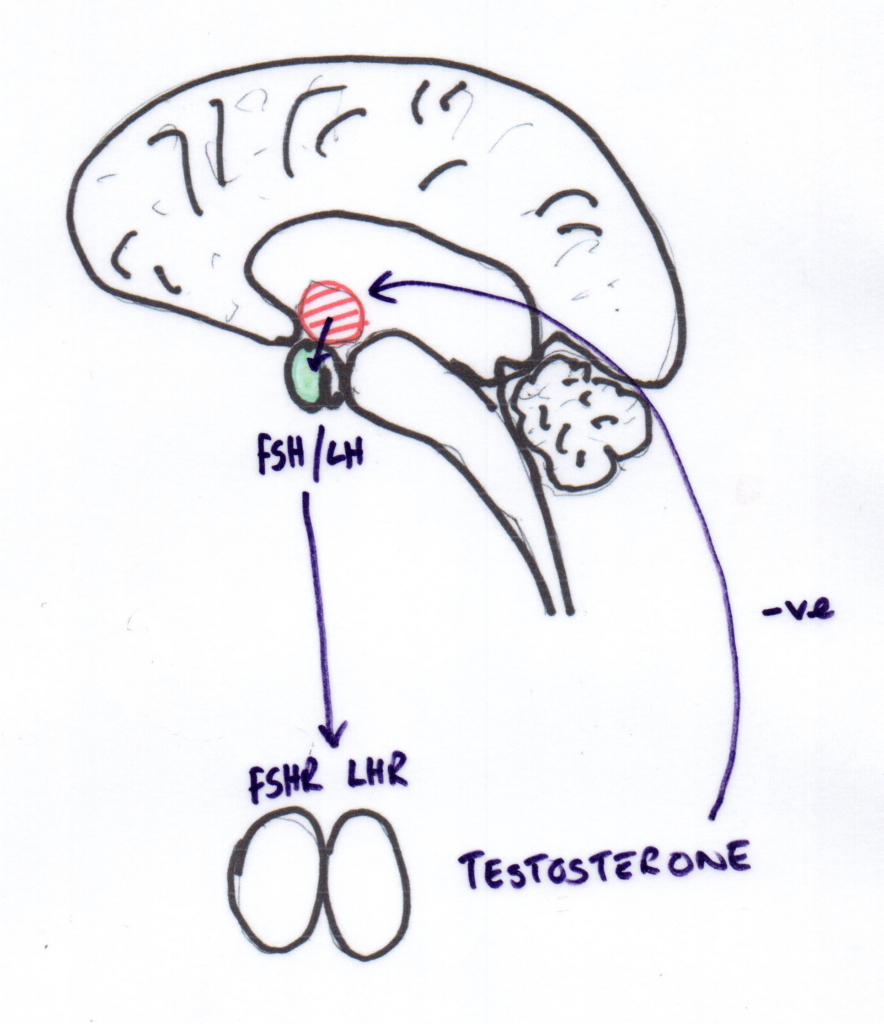
Biological Focus: HPG Axis and LHR
Existing literature suggests possible links between:
- Post-desexing endocrine shifts
- Gonadotrophin signalling
- Connective tissue integrity
For this reason, hypothalamic–pituitary–gonadal (HPG) axis signalling—specifically luteinising hormone receptor (LHR) expression—was selected as a biologically plausible focus for correlation.axis involvement, and specifically luteinising hormone receptor (LHR) expression, was selected as a biologically plausible focus for correlation. Images below show the hormones in an entire patient and a desexed patient.
Evidence and Validation
System Responsiveness Validation (Single-Subject Positive Stimulus Control)
To confirm that RAC event counts reliably separate baseline physiology from a strong activated state under fixed operating parameters, a repeated-measures positive stimulus control was performed using the developer as the test subject (n = 1).
A coffee stimulus was chosen because it is a historically reproducible trigger for pruritus ani symptoms in this individual. Testing was performed under standardised conditions:
- Hardware platform: TC Diagnostic Laser
- Laser: Red
- Delta T: 0.04
- Exposure period: 5 seconds
- Detection threshold setting: 0
- Output: RAC events per 5-second window DAMNIT_V_RAC_Positive_Control_V…
Results (baseline vs stimulus condition):
- Baseline (n=30): Mean 19.8, Median 20, SD 8.9, Range 5–35
- Stimulus (n=40): Mean 74.6, Median 75, SD 9.8, Range 45–90 DAMNIT_V_RAC_Positive_Control_V…
This demonstrated a mean increase of +54.8 events, with an estimated Cohen’s d ≈ 4.9 (very large separation). ROC threshold analysis showed near-complete discrimination between baseline and activated states within this single-subject model:
- >30 events: Sensitivity ~100%, Specificity ~97%
- >35 events: Sensitivity 100%, Specificity 100% DAMNIT_V_RAC_Positive_Control_V…
What this supports
- Strong system dynamic range and signal-to-noise separation under fixed conditions
- Practical justification for the >30 events “strong response” guidance as an operational indicator of marked autonomic activation
Scope limitation
This validation is a single-subject positive stimulus model and demonstrates system responsiveness and within-subject discrimination only. It does not establish population-level diagnostic specificity or clinical causality. DAMNIT_V_RAC_Positive_Control_V…
Download the full validation report (PDF):
System Responsiveness Validation Report – Pruritus Ani Context
Correlation Phase
During the correlation phase, screening outputs indicating HPG-axis reactivity were compared with:
- Surgically confirmed CCr rupture
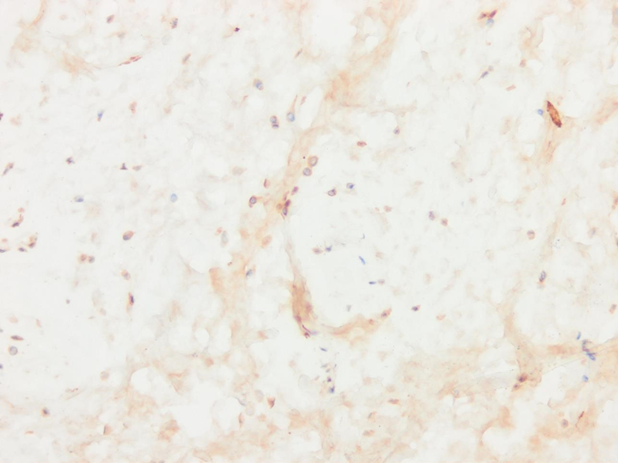
- Immunofluorescent detection of LHR expression in cruciate tissue
This was a correlation study, not a diagnostic validation trial.
The objective was to assess alignment between repeatable functional response patterns and tissue-level biological markers.s whether repeatable functional response patterns aligned with biological markers present in diseased tissue.
H&E stains of normal CCr and Ruptured CCr as reference
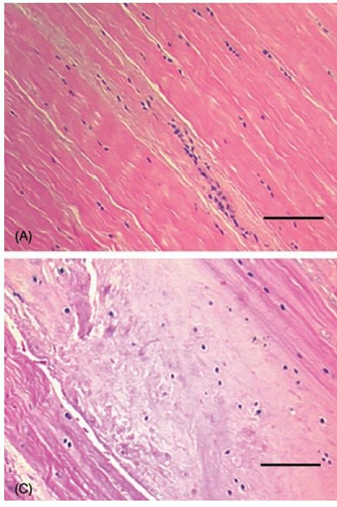
H&E Stain of ruptured CCR in study
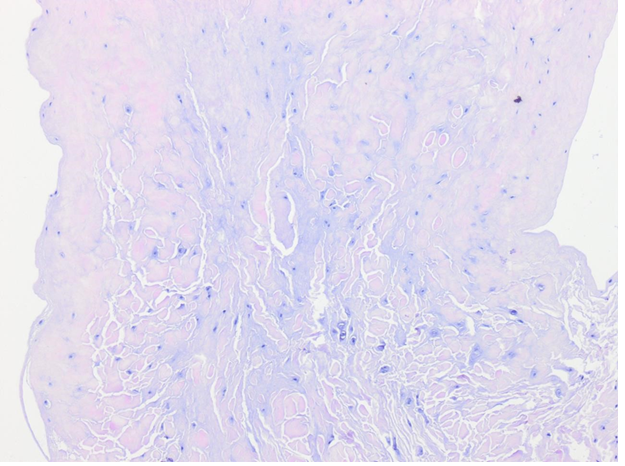
Immunofluorescent LHR stain in ruptured CCr : Score 6/6 based on Kiefel and Kutzler 2020
HPG hormone screen of patient in CCr study
LHR study of the stifle in CCr patient included in the study
Tissue-Level Controls
Samples were obtained only from clinically indicated surgical cases.
A histologically normal cruciate control group was not included because:
- Invasive sampling of healthy cruciate ligaments is not ethically justified
- There is no clinical indication for routine sampling of intact ligaments
Accordingly, the study design was case-referenced rather than case–control at tissue level.
This supports the discussion of correlation but does not allow inference about marker absence in normal tissue.
Longitudinal Observational Cohort (2014–2025)
Design
- Single-practice longitudinal observational cohort
- 11-year monitoring period
- Desexed dogs under routine care
- Post-desexing screening integrated into workflow
Intervention
- Screening for HPG-axis–associated reactivity
- Audio-based exposure protocols
- Adjunct laser acupuncture in reactive cases
- Three-week post-desexing follow-up testing
Primary Outcome
Confirmed cranial cruciate ligament rupture, diagnosed via:
- Clinical orthopaedic examination
- Imaging where indicated
Observed Findings
Over the 11-year period:
- A sustained downward trend in observed CCr incidence was documented within the monitored cohort
- The decline occurred during the period in which screening and modulation protocols were implemented
Early-year variability reflects small cohort sizes.
The relevant finding is the long-term trend.
Scientific Clarification
This dataset:
- Is observational
- Is not randomised
- Was not blinded
- Does not establish causation
- Does not define sensitivity or specificity
- Does not establish predictive validity
It demonstrates longitudinal consistency and feasibility in a real-world clinical setting.
Further controlled, prospective research is required to determine:
- Mechanistic pathways
- Effect magnitude
- Reproducibility
- Diagnostic performance characteristics
What This Evidence Supports
- Long-term integration feasibility
- Internal consistency of application
- Correlation between screening-guided management and observed practice-level outcomes
What It Does Not Support
Replacement of structural diagnostics
Population-level risk reduction claims
Causal inference
Predictive disease prevention claims
Longitudinal Clinical Outcome
Over more than a decade of observation (2014–2025), the practice recorded:
- the number of desexed dogs under active clinical follow-up
- confirmed cases of cranial cruciate ligament rupture
- year-on-year changes within a consistent practice cohort
Observed cranial cruciate ligament disease incidence in desexed dogs monitored within a single veterinary practice (2014–2025).
Data represent observed incidence within the practice cohort. Early-year variability reflects small cohort sizes. The clinically relevant finding is the sustained downward trend over time.
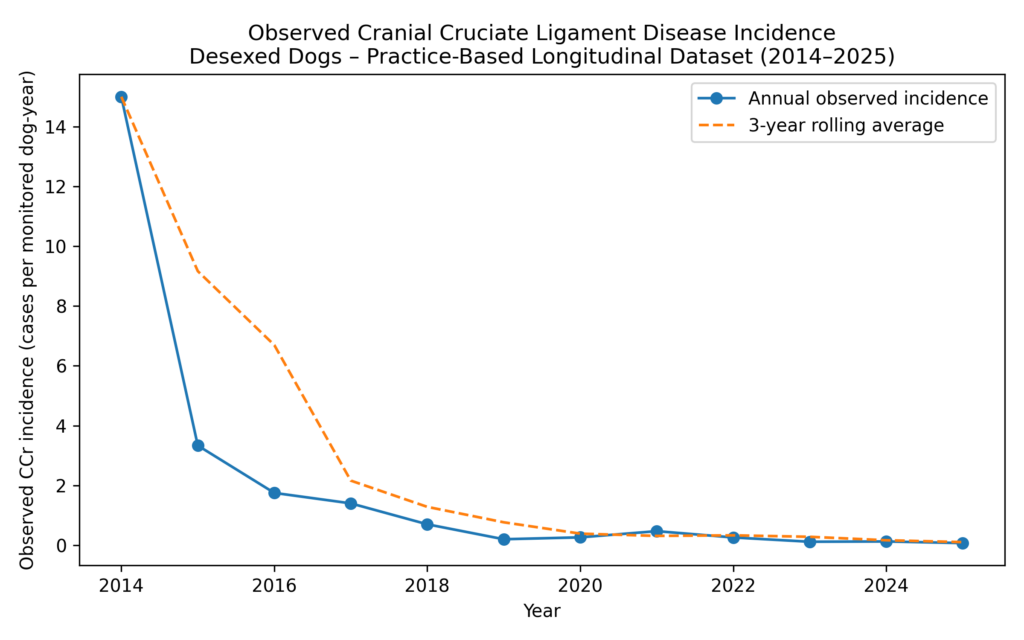
What the Data Shows
The longitudinal data demonstrate:
- a sustained reduction in confirmed CCr disease incidence over time
- this reduction occurring despite an expanding monitored population
- a consistent downward trend when viewed as a rolling average
Early-year variability reflects small cohort sizes and is expected in practice-based datasets.
The clinically meaningful signal is the long-term trend, not isolated annual values.
How to Interpret the Graph
Rates are presented as observed incidence within the monitored cohort, not population risk estimates.
The data demonstrate clinical utility and consistency over time, not proof of causation, prediction, or disease prevention.
Why DAMNIT-V Screen Exists
DAMNIT-V Screen exists because it demonstrated consistent clinical utility within clearly defined scientific boundaries.
It was built in practice, refined through daily use, and designed to support the way experienced veterinarians already think:
Start broadly, narrow carefully, and investigate appropriately.
Explore further clinical uses of the DAMNIT-V Screen, or arrange an in-clinic demonstration via the Contact page.